by Tony Isaacs
For well over half a century we have been promised by mainstream medicine that a cure or major breakthrough for cancer was just around the corner. Every year we see promising new drugs and therapies announced. Yet every year we also see more people contract cancer and more people die of cancer.
Instead of focusing on natural and safe methods of prevention and treatment, we continue to treat by using surgery, chemotherapy and radiation to cut out, poison out and burn out the symptoms of cancer while leaving the underlying causes untreated - and we continue to largely ignore the role that proper diet, nutrition and lifestyle plays in preventing and helping cure cancer.
Although surgery does have some success against a limited number of cancers, chemo and radiation achieve at best a 3% increase in length of survival and true cures from cancer (meaning that the patient becomes completely cancer free and the cancer never returns). The fact is that for those who are diagnosed with cancer, after the third year the survival rate for those who had no treatment at all increases steadily and for those who had mainstream treatment it decreases steadily.
Sources: Dr. Ralph Moss and Webster Kehr, the "Cancer Tutor"
Despite the dismal record, those in the $300 Billion a year cancer industry appear determined to maintain a stranglehold on treatment. One way they do so is to suppress natural alternatives. Another is to misreport their success rates by altering statistics to make their success appear to be much better than it actually is.
Here are six ways that mainstream medicine misreports their statistics:
1. By re-defining "cure" as "alive five years after diagnosis: instead of using the word's real meaning, which is "cancer-free". Thus a patient could still have cancer the entire five years and die one day after the 5th anniversary date of diagnosis and still be recorded as a cure.
2. By simply omitting certain groups of people, such as African Americans, or by omitting certain types of cancer, such as all lung cancers patients, from their statistical calculations.
3. By including types of cancer that are not life-threatening and are easily curable, such as skin cancers and DCIS.
The statistics most commonly reported include many such easily curable cancers, such as localized cancers of the cervix, non-spreading cancers and melanomas, as well as "cancers" that many feel are not true cancers at all, merely pre-cances. For example, DCIS is a pre-cancerous condition that is 99% curable and makes up 30% of all breast cancers. Deduct that 30% from the breast cancer cure rates and survival statistics and and the figures are much less impressive.
4. By allowing earlier detection to erroneously imply longer survival.
5. By deleting patients from cancer treatment studies who die too soon, even if that is on the 89th day of a 90 day chemotherapy protocol.
6. By using a questionable adjustment called "relative survival rate" where they get to deduct a certain number of cancer victims who statistics say would have died during the five years of other causes such as heart attacks, car wrecks, etc.
Source: Tanya Harter Pierce "Outsmart Your Cancer"
These outrageous "fudges", as Ms. Harter too kindly calls them, have all been incorporated into cancer cure statistics to hide the fact that the war on cancer has been hopelessly lost and wrongly waged. In the opinion of many who are far more knowledgeable and qualified than I am, the so-called War on Cancer is little more than a hoax.
"Everyone should know that most cancer research is largely a fraud and that the major cancer research organisations are derelict in their duties to the people who support them." - Linus Pauling PhD (Two-time Nobel Prize winner).
"The National Anti-Cancer Program is a bunch of sh*t." - James Watson, Nobel Laureate for Medicine in 1962 , joint discoverer of the double helix of DNA, and for two years a member of the US Joint Advisory Committee on Cancer
When it comes to mainstream successes, of the three major mainstream treatment methods, surgery is the only one with respectable success rates and even then it is only successful the vast majority of the time in those who have operable types of cancer that has not yet metastisized at the time of diagnosis - and most cancers are not detected prior to metastisizing.
When it comes to Chemo, in the words of Dr. Ralph Moss:
"Chemo has some success in a few kinds of cancer, but in the conventional cancers which chemotherapy sometimes "works" such as small-cell lung cancers, the actual survival benefit is reckoned in weeks or months, not in years. And during this time, the patient is likely to experience major, even life threatening, side effects from the treatment, so the overall advantage to the patient is moot."
Radiation results are even more dismal. In some studies, patients who opted for radiation have had lower survival rates than those who did not have radiation.
Sources: Tanya Harter Pierce, Dr. Rath Foundation
Another common deception of mainstream medicine is to quote "response rates", which is defined as having a 50% tumor shrinkage for a period of twelve months. It has nothing to do with cure rates or long term survival, but it is the statistic that is often quoted to patient by their oncologists.
Yet another deception is the use of the term "remission" to imply cure, when it is nothing of the sort. As "the Cancer Tutor" Webster Kehr writes in "The War Between Orthodox Medicine and Alternative Medicine"
First of all, the National Cancer Institute defines "remission" as:
"A decrease in or disappearance of signs and symptoms of cancer. In partial remission, some, but not all, signs and symptoms of cancer have disappeared. In complete remission, all signs and symptoms of cancer have disappeared, although cancer still may be in the body." NCI - http://www.nci.nih.gov/dictionary/db_alpha.aspx?expand=R What exactly does this definition mean relative to the three "treatment decision criteria" . . . You, the citizen, are supposed to assume that "remission" means a person is cured of their cancer. But that is not what the definition states. It states there is an absence of "signs and symptoms." So is there a correlation between the absence of "signs and symptoms" and the three treatment decision criteria above?
Generally, the determination of remission is based on a reduction in the size of the tumor or in the change of some tumor marker. These things may indicate the number of cancer cells in the body, but they are very, very crude estimates of the number of cancer cells in the body. These numbers also do not measure the pain and suffering of the patient (i.e. the quality of life) or the status of the immunity system, which is very, very important if all of the cancer cells have not been killed.
And then there is what is likely the greatest mainstream deception of all: the millions of people who are diagnosed with cancer, but actually die from the damages done by chemotherapy and radiation, most frequently major organ failure. All of those deaths are recorded as due to cancer. Though that does not bolster the mainstream cancer treatment success rates, it helps hide the dangers and deaths due to mainstream treatments.
It should be plain that the war against cancer is not being won - and to continue to claim otherwise after over half a century begs the question of why such obviously false and misleading claims and statistics. In this respect, one is reminded of the Vietnam War, where we were told that we won every battle and that we killed many more of the enemy in every skirmish. And yet the war was a failure and in the end we admitted it, stopped deceiving the public, and moved on to a different approach to stop the needless loss of lives. Today it appears that the war with Iraq will ultimately end the same way.
The war against cancer has lasted much longer and we have lost millions and millions of lives. After over half a century of failure, one has to ask how long will it take to admit it, stop deceiving the public, and move on to a different approach to stop the needless loss of lives?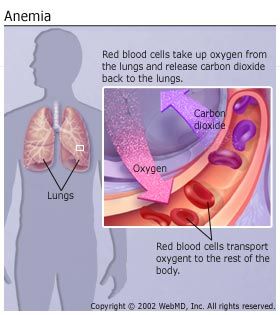 Anemia is a condition that develops when your blood is deficient in healthy red blood cells, which are the main transporter of oxygen to organs. If red blood cells are also deficient in hemoglobin, then your body isn't getting enough iron. Symptoms of anemia -- like fatigue -- occur because organs aren't getting enough oxygen.
Anemia is a condition that develops when your blood is deficient in healthy red blood cells, which are the main transporter of oxygen to organs. If red blood cells are also deficient in hemoglobin, then your body isn't getting enough iron. Symptoms of anemia -- like fatigue -- occur because organs aren't getting enough oxygen. Read more about Anemia Symptoms
Read more about Anemia Symptoms